Timed and Targeted Counselling (TTC)
A family-inclusive behaviour change model
Timed and Targeted Counselling (TTC) is World Vision's family-inclusive behaviour change communication (BCC) approach designed to promote life-saving health and nutrition practices for young children – especially those in the most vulnerable and marginalised households.
TTC empowers families through timely, relevant, and contextualised counselling, delivered using storytelling and dialogue. It aims not only to educate, but to actively engage caregivers and household decision-makers – including fathers and extended family like grandmothers – to create a gender-transformative and supportive environment for child health and development.
Delivered by community health workers (CHWs), guide mothers, or trained volunteers, TTC focuses on the critical early years – particularly the first 1,000 days of life – when children's physical and mental development is most sensitive to positive health behaviours.
Why TTC matters
- Child mortality remains high: Despite a 59% reduction since 1990, 5.4 million children still die annually, with two-thirds of child deaths under age five.
- Most deaths are preventable: An estimated 80% of child deaths are due to causes that can be avoided through improved care-seeking, facility-based delivery, appropriate breastfeeding, child nutrition, hygiene, and responsive caregiving.
- The first 1,000 days are critical: Undernutrition, caregiver stress, disease, poor hygiene, and limited stimulation can cause lasting harm, especially in vulnerable households.
The role of Community Health Workers (CHWs)
CHWs are a proven, cost-effective link between health systems and vulnerable households. Studies show that scaling up CHW-led care could save 3 to 6 million lives over five years, with the greatest gains in Africa.
However, CHWs require better support, legitimacy, and integration into national health systems – challenges that TTC aims to address in line with WHO guidelines on community health.
What makes TTC effective?
TTC overcomes common limitations in health communication by being:
- Timed: Messages are delivered at the right time – aligned with key stages of pregnancy, childbirth, and child development.
- Targeted: Counselling goes beyond mothers to reach entire families, addressing social and gender dynamics that influence decision-making.
- Tailored: CHWs use barrier assessment interviews to understand family context and co-develop practical, achievable solutions.
TTC also prioritises high-risk groups, including adolescent mothers, caregivers facing psychosocial or mental health challenges, and families with limited support systems.
What is the TTC Project Model?
TTC targets families of young children during pregnancy to two years of life, to promote health behaviours, nutrition and early childhood development (ECD). The dialogue-based counselling methodology, and positive and negative stories is based on Home Based Life Saving Skills (HBLSS) method,[1] but has evolved over time. TTC storybooks depict key themes of positive fatherhood, caregiver mental health, and family decision-making for pregnancy and newborn care and nutrition. A review of CHW curricula by the WHO in 2013[2], found TTC to be one of the most comprehensive life-course models. Messages and topics were based on World Vision’s “7-11” strategy[3] for maternal, newborn and child health and nutrition in the 1,000 day period from conception to two years, then updated in 2014 to include ECD, stimulation and play[4] and psychosocial support for maternal mental health,[5] alongside chlorhexidine core care[6], newborn care[7], care for the small baby[8], and the HIV exposed infants.
Now, the 2018 edition takes a flexible approach, improving CHW systems support, and offering a range of optional modules to enable better fit with national CHW systems. During national adoption of TTC in Ghana, Kenya, Lesotho and Sierra Leone, content was created to cover the full range of CHW service packages, to include household health, WaSH, child health (2 to 19 years), and emerging areas of adolescent health, and prevention of violence against children. Content has also been developed for Integrated Community Case Management (iCCM) and support to community treatment of malnutrition.
Alignment with global goals
TTC contributes directly to World Vision’s Our Promise strategy by strengthening CHW systems and promoting sustainable, locally owned health solutions. It also aligns closely with several Sustainable Development Goals (SDGs):
SDG 2.2 By 2030 end all forms of malnutrition, achieving targets on stunting and wasting
SDG 3.1 By 2030, reduce the global maternal mortality ratio.
SDG 3.2 By 2030, end preventable deaths of newborns and children under 5 years of age
SDG 3.3 By 2030, end the epidemics of AIDS, tuberculosis, malaria/communicable diseases
SDG 3.4 By 2030, reduce by one third premature mortality from non-communicable diseases
SDG 4.2 By 2030, ensure access to quality early childhood development, care & pre-primary education
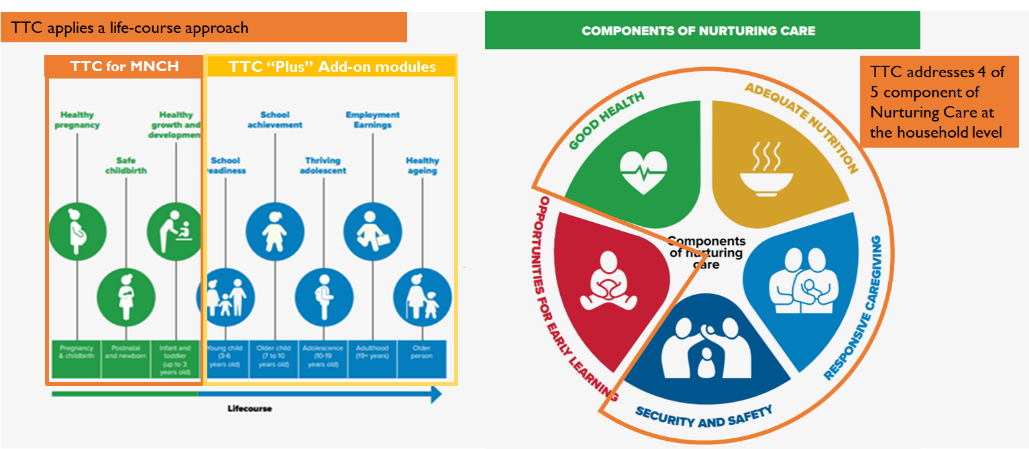
TTC is also aligned with the WHO’s Global Strategy for Women’s, Children’s and Adolescents’ Health (2016-2030) and the WHO Nurturing Care framework, which promotes five interconnected components for child development through a life-course lens (Figure 1).
Figure 1. How TTC aligns to the Nurturing Care Framework
CORE COMPONENTS OF TTC
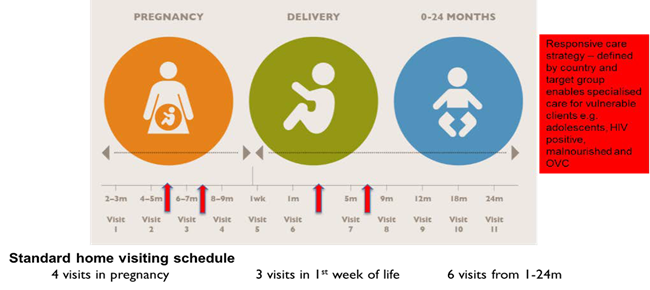
The TTC-HVs conduct home visits for pregnant women to promote antenatal care and planning for skilled care at birth. They visit newborns in the hours and days following birth, identify danger signs and refer appropriately, and advise on appropriate home care for the newborn. They continue to visit families at regular intervals until the child reaches 2 years of age, delivering messages to the family members throughout this important period in the child’s life. In the 2018 edition, HV also conduct routine visits for families of children aged 2-19 years to assess other household and family health issues.
EXPECTED IMPACT
Goals: Improved outcomes for pregnancy and child health, nutrition and child development
Outcomes: Increased adoption of household behaviours, especially improved breastfeeding and complementary feeding practices for young children, care-seeking behaviour and uptake of health services
Target populations: (1) Pregnant women and children under 2 years (including orphans and looked after children). (2) Women and girls of childbearing age to promote health pregnancy timing and spacing and (3) the most vulnerable families who might need additional support.
EVIDENCE BASE
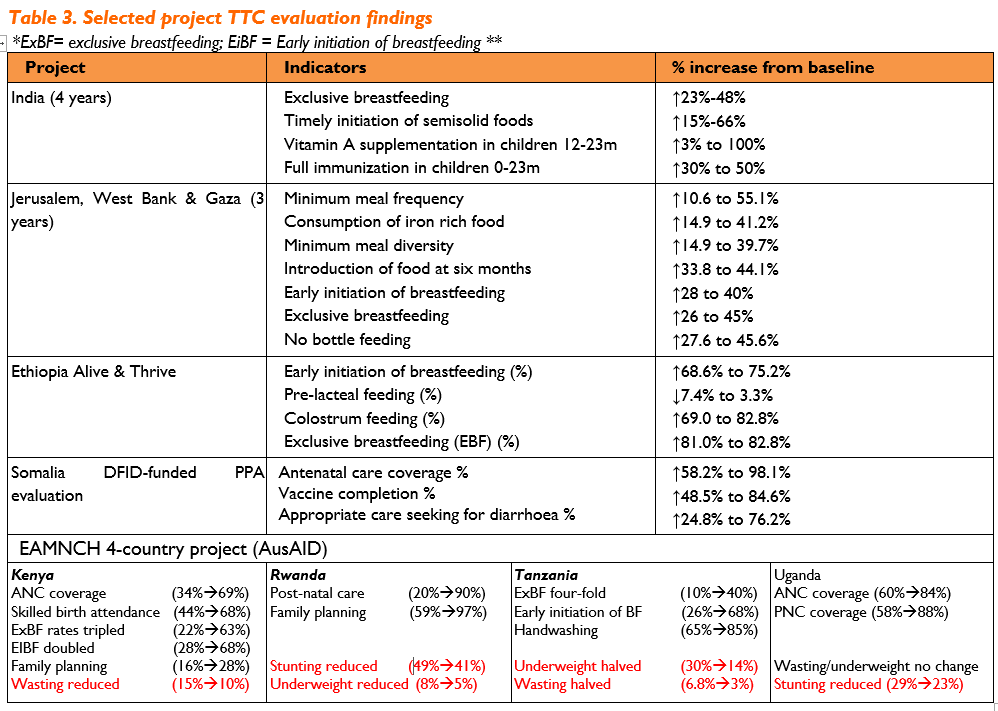
Since its inception in 2010, TTC has been implemented in 38 countries. Evidence includes impact evaluations from 10 countries and research contributing to a diverse portfolio. TTC has demonstrated consistent impact on behaviours determined at the household level such has hygiene, newborn care and appropriate breastfeeding behaviour. TTC’s impact on newborn care and breastfeeding alone contribute to a high estimate of Lives Saved (LiST) and cost effectiveness as demonstrated through research undertaken in Jerusalem and West Bank, and the AIM Health Grant (Table 3). Results from grant-based evaluations include some of the following key findings:
- Pragati study, World Vision India, FHI360 - the four-year USAID-funded Pragati project[10] in India showed improvements across a range of health behaviours, and that family planning more than doubled;
- Ethiopia Alive and Thrive project – TTC delivered by peer mothers found improvement in IYCF practices, reduced need for therapeutic feeding, improved treatment of diarrhoea, in a ‘dose-response’ effect, i.e. more visits led to more improvement. [11] The Ministry of Health approved scale-up in 28 districts.
- A cost-effective scale-up in Palestine - TTC implemented by CHWs found high impact on practices related to newborn care, reduced harmful newborn practices, improved IYCF and care-seeking A cost-effective analysis found a cost per life saved of $197 USD, therefore TTC is highly cost-effective.[12]
- East Africa MNCH grant funded by AusAID - A 3-year TTC/CVA project in Kenya, Uganda, Rwanda and Tanzania, demonstrated consistently positive effects for IYCF indicators across all four countries, wasting/underweight in children was reduced in 3 of 4 countries and stunting reduced in 2 of 4 countries.
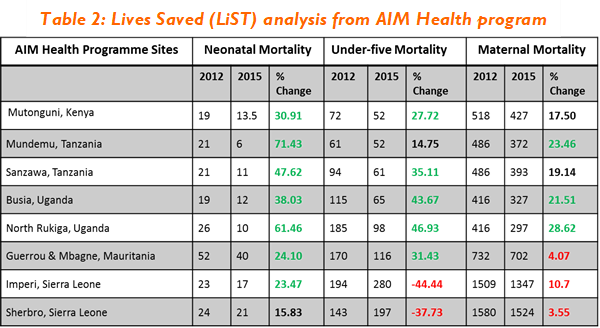
Table 2: Lives Saved (LiST) analysis from AIM Health program
Programme Partnership Agreement (PPA) DFID program – A 6-year DFID-funded programme implemented TTC and CVA in Sierra Leone (SL), Kenya and Somalia, evaluation was further accompanied by a ‘Realist Analysis’ to look at qualitative elements of implementation identified challenges and success-factors such as (1) importance of integration with the National CHW programme (2) loss of fidelity of the model (3) intensive start-up requirements (4) variable targeting of vulnerable groups (5) variable commitment to gender-equity component of TTC (5) High CHW/V workloads and (6) insecurity leading to high turnover and loss of quality in fragile contexts.
- Irish AID Funded AIM Health program - implemented TTC in Kenya, Tanzania, Uganda, Mauritania and Sierra Leone. Exclusive breastfeeding met or exceeded the programme target of 80 percent in all locations with six locations exceeding 90 percent. A Lives-Saved analysis estimated up to 71% and 28% reduction in newborn and maternal deaths (Table 2), except for Sierra Leone during the 2015 Ebola outbreak.[13]
COST PER BENEFICIARY
Costs of TTC are weighted heavily at started up due to training and production of materials. Estimated costs per beneficiary amongst several countries are shown below. The table below shows the estimated cost per child under 5 per year as US$5.36. This can be taken as an estimate of the costs of CHW programme per beneficiary. This data excludes the Palestine project, where cost per life saved was estimated at $197 per life saved, as cost-per-beneficiary in this setting was based on CHWs receiving a full-time salary, which is not the case in any of the other programmes.
IMPLEMENTATION AND SCALE
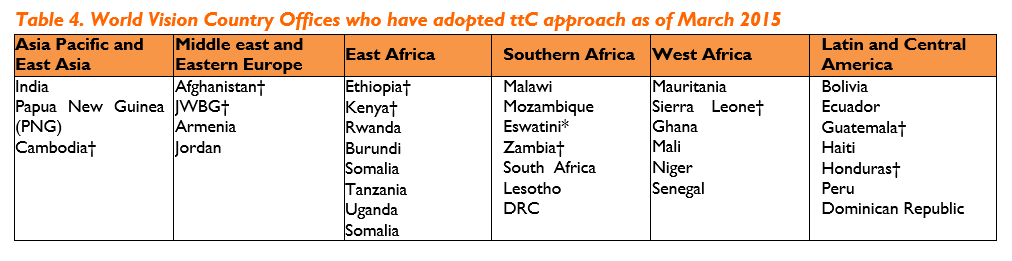
World Vision is currently implementing the TTC model in the following countries (Table 4).
Table 4. World Vision Country Offices who have adopted ttC approach as of March 2015
INNOVATION AND TECHNOLOGY
TTC mHealth Application - The CommCare-based mTTC app enables real-time data reporting, sends reminders for visits and follow up, and includes audio-visuals in local languages and press-play messages. mTTC has been used in 7 countries with 4000 users, and reports show improved quality of data and timely referral.
ICCM integration – Several countries the ICCM have been integrated within TTC and the mTTC app;
Healthy Families – Ghana, Kenya, Lesotho, DRC and Haiti have all included Healthy Families module in TTC
CMAM support and the nutrition root cause assessment – CHWs in Sierra Leone, Mauritania, Ghana all include a root cause assessment at household level for CHWs implementing CMAM support;
Prevention of child marriage – module and storybooks have been developed and being tested in Mauritania;
Prevention detection and reporting of violence against children – a training module, storybooks and referral forms for prevention and referral of VAC has been developed and is being tested in Lesotho and Haiti.
For more information about TTC contact health@wvi.org
[1]Sibley L, Buffington ST, Beck D, Armbruster D (2001). Home based life saving skills: promoting safe motherhood through innovative community- based interventions. J Midwifery Womens Health. 2001 Jul-Aug;46(4):258-66.
[2] Tran et al., 2014 ‘Developing Capacities of Community Health Workers in Sexual and Reproductive, Maternal, Newborn, Child, and Adolescent Health: A Mapping and Review of Training Resources’. PLoS ONE 9(4): e94948.
[3] The 7-11 Start Up Field Guide. http://www.wvi.org/health/publication/7-11-start-field-guide
[4] Lancet Series. ‘Child Development in Developing Countries’ Series 1 (2007) & 2 (2011).
[5] Lancet series. ‘Perinatal Mental Health’. November 14, 2014
[6] Imdad et al. ‘Umbilical cord antiseptics for preventing sepsis and death among newborns’. Cochrane Systematic Reviews 2013, Issue 5. CD008635.
[7] WHO/UNICEF Joint Statement (2009), ‘Home visits for the newborn child: A strategy to improve survival’. WHO/FCH/CAH/09.02
[8] World Health Organisation, ‘Care of the preterm and/or low-birth-weight newborn’.
[9] Nurturing care for early childhood development: a framework for helping children survive and thrive to transform health and human potential ISBN 978-92-4-151406-4 © World Health Organization 2018
[10] World Vision US/USAID (2009) “The Right Messages—to the Right People—at the Right Time” www.wvi.org/sites/.../World%20Vision%20India%20Case%20Study.pdf
[11] Final Evaluation Report: World Vision Alive & Thrive Operations Research (2012) http://aliveandthrive.org/countries/ethiopia/
[12] How many lives did ttC save in Palestine and at what cost? A. Trujillo 2013. http://www.annalsofglobalhealth.org/article/S2214- 9996(15)00922-4/fulltext
[13] Midterm evaluation of the Bonthe AIM health program showed strong positive trends up to 2014, however the ebola epidemic dramatically cut uptake of health services at facilities, which had a strong negative impact on the Lived Saved findings.
[14] Chou, Victoria B et al. “Expanding the population coverage of evidence-based interventions with community health workers to save the lives of mothers and children: an analysis of potential global impact using the Lives Saved Tool (LiST).” Journal of global health vol. 7,2 (2017): 020401.
Tools

Publications